

Some cool Weight loss images:
Famine Memorial – Dublin

Image by infomatique
multitext.ucc.ie/d/Famine
How many died?
Because data are poor, historians arrive at different estimates of the number that died. In the period 1846–1851 between 1,000,000 and 1,500,000 people died: we cannot be certain of the number. Besides, births and marriages dropped significantly. Those hardest hit were the agricultural labourers, the class that had increased most rapidly in numbers in the decades before the Famine. As Karl Marx stated, ‘The Irish famine of 1846 killed more than 1,000,000 people, but it killed poor devils only’ (Capital, i, pt vii, chapter 25). The poor were the first and the most to die. The unprecedented scale of deaths was not due to starvation alone: infectious diseases such as typhus, relapsing fever, and cholera, killed very many.
Famine deaths and diseases
Starvation is a slow killer. First the body uses up all its deposits of fat. The metabolic rate sinks and physical and mental activity declines. Blood pressure falls. The internal organs, including the intestines, degenerate. The skin grows paper-thin, dull, grey and blotchy. Fluid is retained in the body (famine oedema). Normally, one-third of body weight is lost before death occurs. The final stages are uncontrolled diarrhoea and cardiovascular collapse. Children under the age of five are particularly vulnerable. They suffer from muscle waste, a wizened and shrunken appearance that makes them look like old men and old women, swelling of the abdomen and lower limbs, lesions and darkening of the skin, and diarrhoea. Reports describe these conditions:
… a vast number of impotent folk, whose gaunt and wasted frames and ghastly, emaciated faces were too obvious signs of the suffering they had endured. The little boys and girls presented a hideous sight. In many instances, their heads had become bald and their faces wrinkled like old men and women of seventy or eighty years of age. [Thomas Armstrong, My life in Connaught (London 1906) 13; repr. in L. A. Clarkson & E. Margaret Crawford, Feast and famine: a history of food and nutrition in Ireland, 1500–1920 (Oxford 2001) 140]
… We entered a cabin. Stretched out in one dark corner … were three children huddled together, lying there because they were too weak to rise, pale and ghastly, their little limbs … perfectly emaciated, eyes sunk, voices gone, and evidently in the last stages of actual starvation. On some straw … was a shrivelled old woman, imploring us to give her something,—baring her limbs partly, to show how the skin hung loose from the bone. [William Bennett, ‘Extracts from an account of his journey in Ireland’, Transactions of the Central Relief Committee of the Society of Friends during the Famine in Ireland 1846 and 1847 (Dublin 1852) 163; repr. Clarkson & Crawford, ibid.]
With hunger came the vitamin deficiency diseases: scurvy, pellagra and xerophthalmia that get worse the longer hunger continues. Scurvy is caused by deficiency of vitamin C. Symptoms are swollen bleeding gums with loosened teeth, soreness and stiffness of the joints and lower extremities, excruciating pain, bleeding under the skin and in deep tissues, and eventually death by haemorrhage. It had been rare in Ireland because potatoes have adequate vitamin C. Now it became common. Sudden deaths of workers on relief schemes can be attributed to scurvy. Pellagra, caused by a deficiency of niacin (part of the vitamin B complex), is characterised by dermatitis, diarrhoea, and dementia. This was caused by malnutrition, mostly over-dependence on a relief diet of Indian corn. Xerophthalmia is an eye disease associated with vitamin A deficiency and malnutrition in general. Children aged from three to five are particularly vulnerable. Symptoms are night blindness and, later, ulceration of the cornea, leading to blindness. All these conditions are reported during the Famine.
In famines, most people do not die of hunger but of hunger-related fevers and diseases. The most important of these are typhus, relapsing fever, dysentery, and cholera.
Epidemic typhus is caused by the bacterium Rickettsia prowazekii, which is carried by the human body louse (Pediculus humanus; Irish míol cnis). Lice become infected by feeding off an infected human: there is no known animal reservoir. When infected lice feed on a human, they may defecate. When the person scratches the bite, the faeces (which carry the bacteria) are scratched into the wound or into the mucous membranes. Typhus can also be caught by inhaling the faecal dust of lice in bedding and clothing. The incubation period is seven days. Symptoms are headache, coughing, muscle pain; abrupt onset of high fever, chills, prostration; and mental confusion. By the sixth day, a rash appears on the trunk and spreads, and may become haemorrhagic and necrotic. Other common manifestations are delirium, photophobia, eye pain, kidney failure and enlargement of the spleen. Without modern treatments, nearly 100% of patients die of the disease in epidemic conditions.
Louse-borne relapsing fever is caused by the spirochete bacterium Borrelia recurrentis. No animal reservoir exists: pediculus humanus is the vector. The louse feeding on infected humans acquires the bacterium which then multiplies in the gut of the louse. The louse bite itself will not transmit the bacterium to another person. When an infected louse feeds on an uninfected human, the organism gains access when the victim crushes the louse or scratches the area where the louse is feeding. Borrelia recurrentis infects the patient either through the scratches or through mucous membranes (including nasal ones) and then invades the bloodstream. The incubation period is 2 to 14 days. The patient develops a sudden-onset high fever. The initial episode usually lasts 3–6 days and is usually followed by a single, milder episode. The fever episode may end in a “crisis”—shaking chills, followed by intense sweating, falling temperature, and low blood pressure. This stage may result in death After several cycles of fever, patients may develop dramatic central nervous system symptoms such as seizures, stupor, and coma. The disease may also attack heart and liver tissues, causing inflammation of the heart muscle (myocarditis) and inflammation of the liver (hepatitis). Diffuse bleeding and pneumonia are other complications. Mortality rates from 30 to 70% are reported in untreated patients during epidemics.
Typhus and relapsing fever spread rapidly where there is poor hygiene and where lice-infested starving people crowded together in workhouses, fever hospital, feeding centres, and crowded ships without sanitation; and in the squalid, decrepit, and hideously over-crowded urban areas to which famine victims fled. Unwashed clothing and bedding are an ideal environment for the proliferation of lice. Irish mortality rates are those typically reported for untreated typhus and relapsing fever epidemics.
Dysentery is an illness involving severe diarrhoea, often with bloody faeces, vomiting, septicaemia, and fever. It is caused by the bacterium Shigella dysenteriae and is highly contagious. It is a major threat in crowded areas with inadequate sanitation, poor hygiene, and bad water because it is spread by faecal contamination, whether by personal contact or water-borne. Epidemic dysentery is fatal in about 5–15% of cases—particularly to children, the elderly, and the under-nourished. Deaths from dysentery rose sharply in 1846–7, and remained high until 1849.
Cholera appeared in 1849. It is an acute diarrhoeal disease caused by infection of the intestine by the bacterium Vibrio cholerae. When the infection is severe it is characterised by profuse watery diarrhoea, vomiting, and leg cramps. Rapid loss of body fluids leads to dehydration and shock. Without treatment, death can occur within hours. The disease is got by drinking contaminated water or eating contaminated food. In an epidemic, the source is usually the faeces of infected persons and cholera spreads rapidly where there is inadequate treatment of sewage and drinking water. Its effects were most severe about the ports. It was the principal killer after typhus and relapsing fever.
Mortality from other diseases—especially tuberculosis, measles, scarlet fever—rose rapidly in a population whose immune system was lowered by hunger and exposure.
Donnchadh Ó Corráin
23 January 2006
Image from page 1333 of “Rational hydrotherapy : a manual of the physiological and therapeutic effects of hydriatic procedures, and the technique of their application in the treatment of disease” (1902)
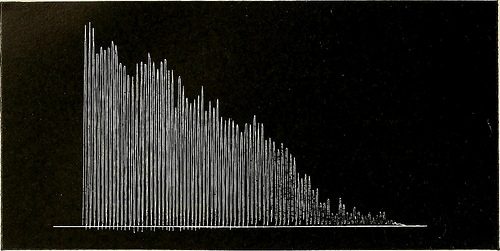
Image by Internet Archive Book Images
Identifier: rationalhydrothe00kell
Title: Rational hydrotherapy : a manual of the physiological and therapeutic effects of hydriatic procedures, and the technique of their application in the treatment of disease
Year: 1902 (1900s)
Authors: Kellogg, John Harvey, 1852-1943
Subjects: Hydrotherapy Hydrotherapy
Publisher: Philadelphia, : F.A. Davis Co.
Contributing Library: Francis A. Countway Library of Medicine
Digitizing Sponsor: Open Knowledge Commons and Harvard Medical School
View Book Page: Book Viewer
About This Book: Catalog Entry
View All Images: All Images From Book
Click here to view book online to see this illustration in context in a browseable online version of this book.
Text Appearing Before Image:
S., was a young man aged 21, weight140 lbs. The normal amount of tidal air was determined to be43 cubic inches. The patient was placed in an immersion bathat 108°. At the end of twelve minutes, the amount of tidal airwas found to be 27 cubic inches. Ten minutes after the bath, thetidal air was 33 cubic inches; 30 minutes after, 37 cubic inches.This experiment shows a loss in the volume of the respired airamounting to 37.5 per cent. {d) A wet-sheet rub at a temperature of 40° was administeredtoa young man, O. R. C, aged 25, weight 142 lbs. The initialvolume of tidal air was 28 cubic inches. The volume of tidal airimmediately after the treatment was 35 cubic inches, an increaseof nearly 26 per cent. (c) The subject, F. J. W., was a young man aged 25, weight127 lbs. The initial volume of tidal air was ^t, cubic inches.Cold mitten friction was administered at 45° for two minutes.Immediately after the application the tidal air was found to be51 cubic inches, an increase of 55 per cent.
Text Appearing After Image:
Fig. 256 (Exp. 45). Ergogram Obtained by Means of Mossos Ergograph, Showingal Iatigue Curve of a Younjj Man, R. A. S. Total work, 4.994 kgm. (p. 1123). Fig. 257 (Exp. 45). Ergogram Showing Fatigue Curve of R. A. S. after a Spray at 113°for Fifteen Minutes. Total work, 4.432 kgm. (p. 1123).
Note About Images
Please note that these images are extracted from scanned page images that may have been digitally enhanced for readability – coloration and appearance of these illustrations may not perfectly resemble the original work.
Success: After Weight Loss Surgery 2008 – Charlotte, NC

Image by kevin_d_old
Taken at the 2008 "Success: After Weight Loss Surgery" conference in Charlotte, NC hosted by Southeast Bariatrics in association with www.band2gether.net.




















